By Ashley Kurzweil and Jamie Floyd
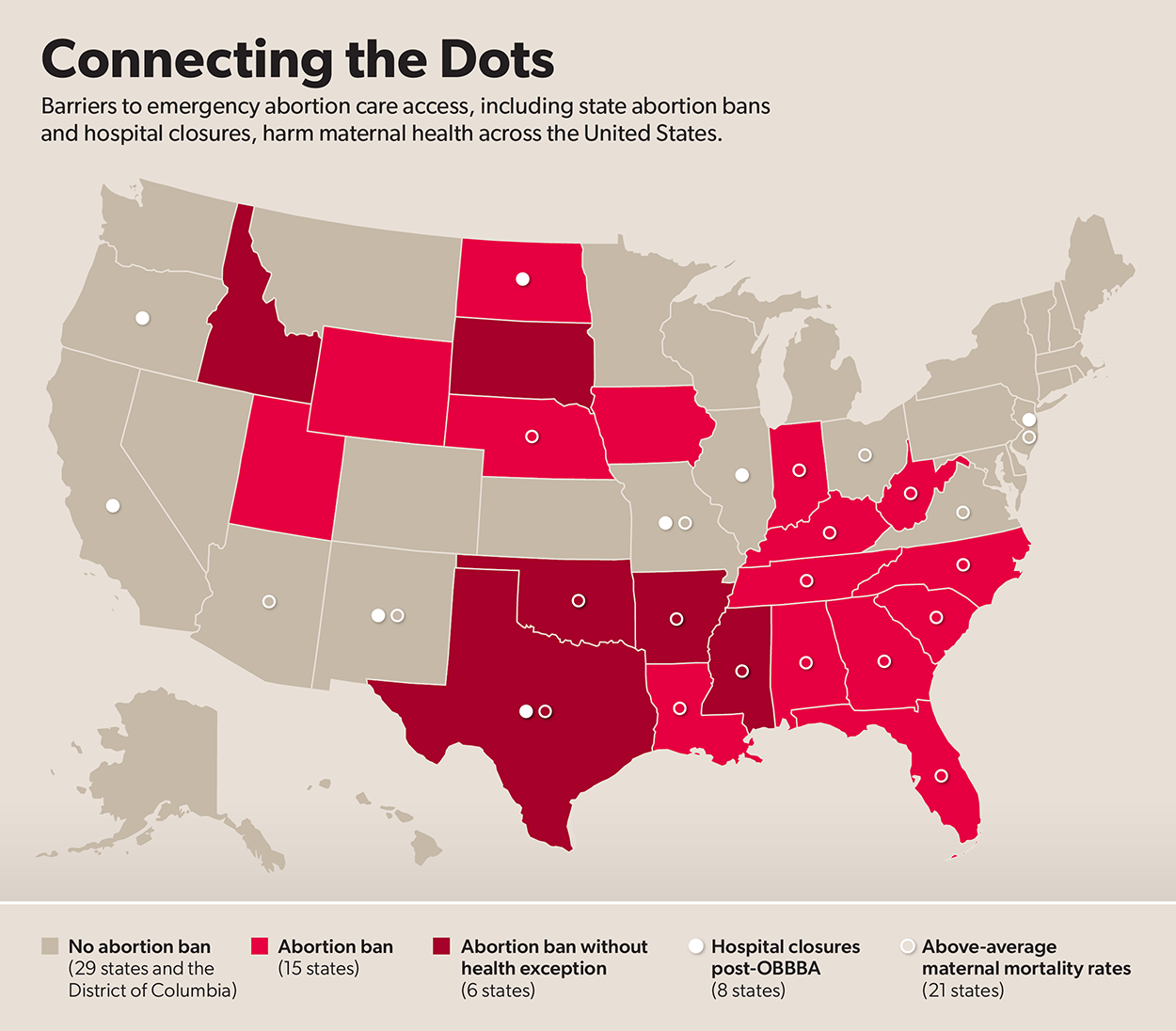
Sources: Maternal Deaths and Mortality Rates per 100,000 Live Births, KFF, https://www.kff.org/state-health-policy-data/state-indicator/maternal-deaths-and-mortality-rates-per-100000-live-births/ (last visited Mar. 31, 2026); Policy Tracker: Exceptions to State Abortion Bans and Early Gestational Limits, KFF (Nov. 24, 2025), https://www.kff.org/womens-health-policy/exceptions-in-state-abortion-bans-and-early-gestational-limits/.
All people deserve access to the abortion care they need, including pregnant people experiencing a medical crisis who need abortion care as emergency treatment. At least one-third of pregnancies involve emergency room visits. And up to 15% of pregnancies include life-threatening conditions during the first trimester. In spite of these clinical realities and the ongoing maternal health crisis, anti-abortion politicians have made it more dangerous to be pregnant in the United States—especially for women of color and women in rural areas. State abortion bans, attacks on federal emergency care protections, and hospital closures in the wake of the One Big Beautiful Bill Act (OBBBA) have compromised access to emergency abortion care and are forcing people to continue pregnancies that put their health and lives at risk.
In light of these threats, advocates, health care providers, and policymakers must come together to comprehensively address abortion access and maternal mortality. These issues are interconnected and require multifaceted policy solutions, with the ultimate goal of improving access to all reproductive health and pregnancy care.
Federal Emergency Care Protections Under Attack
For the last 40 years, the Emergency Medical Treatment and Active Labor Act (EMTALA) has required U.S. hospitals to provide stabilizing treatment to people in emergencies, including providing abortion care. Pregnant people can experience various medical complications for which abortion might be the necessary stabilizing treatment, including preterm premature rupture of membranes, severe preeclampsia, and ectopic pregnancies, among other conditions.
However, post-Dobbs v. Jackson Women’s Health Organization state abortion bans have interfered with the implementation of these federal protections. Abortion bans in states including Arkansas, Idaho, Mississippi, Oklahoma, South Dakota, and Texas lack exceptions for the health of the pregnant person. The Constitution makes clear that federal laws like EMTALA override state abortion bans that do not include an exception when the health and life of the pregnant person are at risk. The Biden Administration issued guidance in July 2022 reaffirming hospitals’ obligations under EMTALA to provide necessary emergency abortion care. However, health care systems and providers have struggled to implement the requirements of EMTALA given the legal risks and uncertainties abortion bans have introduced. The Trump administration made matters worse in June 2025 when it rescinded the Biden-era EMTALA guidance.
Both the Supreme Court and the Trump administration have failed to defend longstanding EMTALA emergency care protections. In June 2024, the Supreme Court refused to settle the question of whether and when health- and life-saving emergency abortion care is allowable in states where abortion is banned with no exceptions for preserving the health of a pregnant patient. And in March 2025, the Trump Administration dropped an ongoing federal lawsuit against the state of Idaho that sought to ensure hospitals provided emergency abortion care. In response, St. Luke’s Health System took up the legal fight and sued the state of Idaho for failing to enforce EMTALA requirements. In March 2025, a federal district court ruled that Idaho must allow St. Luke’s Health System to provide emergency abortion care as the case proceeds.
Tierra’s Lived Experience: Consequences of Delays and Denials of Emergency Abortion Care
Anti-abortion policies endanger the lives and health of pregnant people, resulting in preventable deaths and suffering. Across the country, pregnant people have been turned away from hospitals, unable to get the life-saving emergency care they need. Some have been forced to beg hospitals or courts for that care. And far too many have experienced irrevocable health complications and fertility loss. The individual stories highlighted in this resource represent the countless experiences of women denied abortion care in the U.S.
Tierra Walker was described by her teenage son as a protector, friend, coach, and his closest friend. She experienced pregnancy while living with diabetes and high blood pressure. Tierra lived in Texas, which bans abortion. Knowing she was at high risk of developing preeclampsia, she asked her doctor for abortion care, but her doctor said there was no emergency. More than 90 physicians were involved in her care, but none of them discussed abortion care. At 20 weeks pregnant, her teenage son discovered Tierra on her bed after passing away from preeclampsia. Tierra’s aunt said, “They didn’t want to offer to end the pregnancy, because the government or someone says you can’t? So you’d rather let somebody die? Now we are the ones that have to suffer.”
Barriers To Emergency Abortion Care
State abortion bans with criminal penalties for providers and unworkable medical exceptions have created a chilling effect on the provision of emergency abortion care, resulting in delays and denials. Abortion bans put pregnant people’s future fertility, health, and lives at risk. In practice, both health and life exceptions to abortion bans have proven to interfere with providers’ ability to offer the standard of care, which often leads to pregnant people suffering because their medical condition must deteriorate to a point of extreme risk before meeting a statutory exception and receiving stabilizing treatment. While EMTALA is still the law of the land, fear of legal repercussions and ambiguity in the interpretation and application of federal and state guidance on how to treat pregnant patients in emergency situations can limit providers’ ability to provide care. One study found that states with abortion bans that lack health exceptions had more obstetric-related EMTALA violations – or confirmed cases in which patients did not receive the emergency care they were entitled to under EMTALA – compared to less restrictive states.
The recent rise in hospital closures due to Medicaid cuts in the OBBBA worsens the inaccessibility of emergency abortion care. Patients often receive emergency abortion care in hospital emergency rooms, obstetric emergency departments, and labor and delivery units. When those units shutter, patients must travel outside their communities to seek emergency abortion care. The logistical and financial obstacles that come with the need to travel greater distances for care can be prohibitive and dangerous. The National Partnership for Women & Families found that 12 hospitals have closed since the enactment of OBBBA. More closures are expected to follow as the law’s implementation continues into 2027.
While obstacles to emergency abortion care harm all communities, they particularly impact women of color and women in rural areas. Research from the National Partnership shows that Black women and women in rural areas are especially likely to live in states that ban abortion. And Latina women are the largest group of women of color living in states that ban abortion. Additionally, OBBBA is expected to severely impact rural communities. National Partnership analysis indicates that 131 rural hospitals across the country with labor and delivery units are at risk of closure or severe service cutbacks.
Rachel’s Lived Experience: Consequences of Delays and Denials of Emergency Abortion Care
Rachel Harrison experienced previable preterm premature rupture of membrane during two separate pregnancies, and in both instances, Catholic hospitals denied her emergency abortion care. Despite living in California, where abortion is legal and hospitals are required to provide stabilizing care in emergency situations, providers denied her abortion care and she had to travel to other hospitals. During her first pregnancy, a provider said that the hospital could do nothing. And in her second pregnancy, the staff said fetal cardiac activity prevented them from providing abortion care despite Rachel experiencing sepsis. Rachel is now suing Catholic Health System for denying her emergency abortion care.
Lack of Access to Emergency Abortion Care Harms Maternal Health
Structural barriers to emergency abortion care are especially egregious in light of the ongoing maternal health crisis. In the United States, two to three women die each day from causes related to pregnancy, and many more experience serious or life-threatening pregnancy-related complications. Black and Indigenous women face the greatest risk of maternal death. Compared to their white counterparts, Indigenous women are twice as likely and Black women are 3.5 times more likely to die from pregnancy-related causes.
Denying pregnant patients appropriate emergency medical treatment places them at heightened risk for severe adverse health consequences. In the short term this includes hemorrhage, infection, and death. In the long term, loss of fertility, chronic pelvic pain, heart attack, and stroke. Access to emergency abortion care is critical for pregnant people from communities experiencing systemic oppression, who often face barriers to necessary prenatal and preventive care and are in turn more likely to visit emergency rooms. When pregnant people cannot access adequate primary or prenatal care, they are more likely to develop underlying conditions that make pregnancy more dangerous.
Barriers to emergency abortion care, including abortion bans and violations of EMTALA, have devastating consequences for pregnant patients’ health outcomes. Women living in states that ban abortion are significantly more likely to die during pregnancy, while giving birth, or soon after birth, compared to those who live in states where abortion is legal and accessible. Abortion bans are particularly dangerous for Black women; Black women living in states that ban abortion are 3.3 times more likely to die than white women in those same states. The research indicates this breakdown is likely due to provider uncertainty over whether to follow EMTALA obligations or their state abortion restrictions.
Alarmingly, 40 percent of OB-GYNs in states with abortion bans reported that bans constrain their ability to provide care for miscarriages and pregnancy-related emergencies. This legal uncertainty and fear of criminal penalties have driven providers to relocate out of restrictive states. Provider shortages and rising hospital closures will only compound maternity care deserts. Women in these communities already receive less prenatal care and have worse health outcomes. Given the ongoing erosion of abortion access, the provider workforce, and our health care system, it is no coincidence that states with barriers to emergency abortion care have above-average maternal mortality rates. Restricting access to emergency abortion care will continue to exacerbate the maternal health crisis in the U.S.
Candi’s Lived Experience: Consequences of Delays and Denials of Emergency Abortion Care
Candi Miller was a mother of three in Georgia and known for nurturing gardens and caring for stray cats. Candi lived with lupus, diabetes, and hypertension, and doctors warned that having another baby might kill her. When she became pregnant again, she was afraid to seek care amid her state’s abortion ban. Georgia bans abortion without a health exception that accounts for chronic conditions that present fatal risks. Candi’s family said she didn’t visit a doctor amid health complications “due to the current legislation on pregnancies and abortions.” Candi passed away in her home with her three-year-old daughter by her side.
The National Partnership for Women & Families honors Tierra, Rachel, Candi, and their loved ones, and will continue to fight for the autonomy of pregnant people to control their bodies and exercise reproductive freedom.
A Call for Change
Extremist politicians are putting pregnant people’s lives at risk by undermining access to emergency abortion care. We need state and federal lawmakers to ensure that pregnant people can get the health services they need and that providers will not be punished for following the standard of care. In response to the threats to EMTALA and the risks of the post-Dobbs legal landscape, states including Illinois, Colorado, and California have passed legislation to reaffirm protections for emergency abortion care. While EMTALA already provides federal safeguards, enshrining emergency abortion care protections at the state level is important to prevent further tragedy. Additionally, we urge state and federal lawmakers to use their oversight authority to probe EMTALA compliance issues regarding delays and denials of emergency abortion care. Federal lawmakers must hold the Centers for Medicare & Medicaid Services (CMS) accountable for enforcing EMTALA for pregnant patients facing medical crises and investigate EMTALA complaints involving delayed or denied emergency abortion care.
Barriers to abortion care harm all of us, including people experiencing pregnancy, childbirth, and postpartum. Recognizing how attacks on abortion care fuel the maternal health crisis and working to address the issues in tandem are essential. Pregnant and birthing people must have full access to reproductive health and pregnancy care to live healthy and safe lives. It’s incumbent on all of us—advocates, policymakers, providers, and individuals—to fight for these changes.
Pregnant and birthing people deserve a healthcare system responsive to their needs at all stages of their lives and health. This includes high-quality care that is culturally and linguistically accessible, public and private insurance coverage that provides affordable access to services, and access to diverse medical professionals capable of meeting the needs of patients. It also includes mitigating the impact of Medicaid cuts and extending premium tax credits. Abortion is essential health care. No one should have to worry about whether their doctor will deny or delay health- or life-saving emergency abortion care because of political interference. No person should die because their doctor is afraid to provide needed care.
The authors are grateful to Saranya Kasinathuni, Kacey Napper, Josie Hwang, MacKenzie Burgoyne, Kylie Foster, Amani Echols, Jaclyn Dean, Mettabel Law, Nan Strauss, Erin Mackay, Rosann Mariappuram, and Nima Sheth for their contributions.
 Kamala Harris at NPWF’s 2017 Gala Dinner")








